")
Original Article
Etiological Evaluation of Primary Amenorrhea In A Rural Teaching Hospital
Asma Akhtar1, *Sunita Sudhir2
1Junior Resident, Dept. of OBG, Kamineni Institute of Medical Sciences, Narketpally 2Professor, Dept. of OBG, Kamineni Institute of Medical Sciences, Narketpally
*Corresponding Author
Sunita Sudhir P
Professor of OBG,
Department of OBG,
Kamineni Institute of Medical
Sciences, Narketpally, Nalgonda,
Telangana State - 508254
Email Id: psunitasudhir@gmail.com
Abstract
Introduction: Menstruation is the physical herald to physiologic capacity of conception. Attainment of menarche in a girl brings a lot of confidence and feminism in a girl. Though the incidence of primary amenorrhea is less than 1%, it accounts for significant amount of psychological trauma. In the present day scenario, there are a lot of treatment modalities which can at least restore her menstrual functions, and prevent complications.
Objectives: To determine various causes of primary amenorrhea in a rural Medical College and to emphasize general approach to primary amenorrhea.
Materials and Methods: A retrospective study was performed using 15 complete medical records of women with primary amenorrhea who attended Gynecology OPD, Department of Obstetrics & Gynecology, from June 2016 to June 2018. Cases were analyzed according to clinical profile, development of secondary sexual characters, physical examination, pelvic and rectal examination, hormone profile, pelvic USG, MRI and cytogenetic study including karyotype.
Results: The most common cause of primary amenorrhea was Mullerian anomalies (60%) in present study. There were 2 cases of early gonadal failure, 1 case of pure gonadal dysgenesis, 1 case of Turner mosaic, 1 case of Androgen insensitivity syndrome and 1 case of congenital adrenal hyperplasia.
Conclusion: In this study, Mullerian anomaly was the most prevalent etiological factor leading to amenorrhea followed by premature ovarian failure. However, this was a small scale study and larger study group study must be needed. Racial, genetic and environmental factors could play role in the cause of primary amenorrhea.
Introduction
Amenorrhea is absence of menses in women of reproductive age. Primary amenorrhea (PA) is defined as theabsence of menarche by the age of 14 without the development of secondary sexual features or lack of menstruation bythe age of 16 despite the existence of features. 1 Secondary amenorrhea is normal growth with the appearance of secondary sexual characterized as no menses for an interval of time equivalent to a total of at least
three previous cycles, or in a previously irregular menses for six months. 2According to World Health Organization estimates, amenorrhea stands as sixth largest major cause of female infertility and affects 2- 5% of all women in the child bearing age. 3 The prevalence of primary amenorrhea is less than 1%. 4 The incidence is increasing better utilisation of healthcare, declining-trend in child marriage and increased awareness due to social media.5 In fact, amenorrhea is a symptom rather than a disease that results due to several different causes. The main reasons include improper functioning of ovaries, absence of uterus and vagina, hormonal imbalance, excess of male testosterone, and endometritis.6 There are studies from various regions of the world on aetiology of primary amenorrhea. The two main causes are because of increased reporting, Mullerian anomalies and gonadal dysgenesis with different frequencies in different parts, some have shown anatomic abnormalities
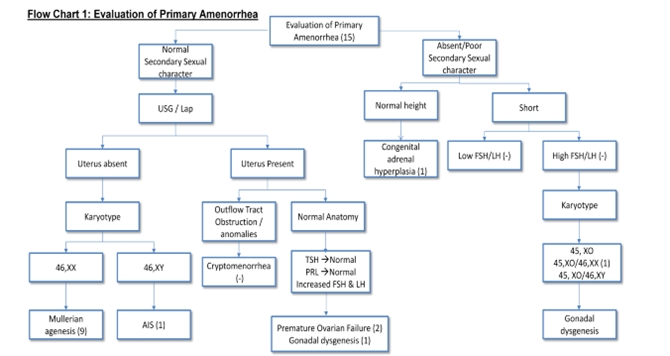
as the most common cause while others have reported gonadal failure as the commonest one.10-13 We carried out a retrospective study, with the purpose of establishing the frequency and the type of different etiological factors among patients with primary amenorrhea. (FLOW CHART 1). A case of primary amenorrhea should be evaluated thoroughly as it has impact on both physical and psychological well being of the patient.7 Early diagnosis and timely intervention is necessary to prevent long term health and social consequences.8 As soon as the aetiology is established in a particular case, the patient can be counseled regarding the prognosis and future fertility options.9
Material and Methods:
The present study was a retrospective study conducted in the Department of Obstetrics and Gynaecology. All cases of primary amenorrhea who attended the Gynaecologic OPD from June 2016 to June 2018 were included in the study. The data was collected based on the medical records of the patients. As it was a retrospective study, ethical clearance was exempted as per hospital policy. There were a total of 15 cases of primary amenorrhoea registered over a period oftwo years (June 2016 to June 2018).
The workup of primary amenorrhea included the following:
History: Patients were asked about their eating habits, exercise patterns, their weight, medication use, presence of galactorrhoea and symptoms of androgen excess, abnormal thyroid function, or vasomotor instability. History was elaborated regarding withdrawal bleeding to progesterone or estrogen & progesterone, any systemic illness, history of tuberculosis. Family history of primary or secondary amenorrhea, mental retardation, any other significant illness was also elicited.
Examination: Physical examination included examination of height, weight, built, BMI (body mass index), presence of secondary sexual characters, thyroid palpation, Tanner staging of breast and pubic hairs, local examination of external genitalia were done. Rectal and/or pelvic examination was done to assess anatomic or Mullerian anomalies. Presence of Dysmorphic features such as a webbed neck, low hairline and other features of Turner syndrome were recorded.
Laboratory Investigations: The initial workup included serum luteinizing hormone, follicle- stimulating hormone, prolactin, and thyroid- stimulating hormone levels, serum free and total testosterone and dehydroepiandrosterone sulphate, estradiol and 17-OHP. A complete blood count and comprehensive metabolic panel, Mantoux test and X-ray of chest was done if history or examination was suggestive of chronic disease. Pregnancy test was done wherever necessary. Pelvic ultrasonography (transabdominal or transvaginal) was done for presence of uterus, adnexae, and any reproductive tract anomaly.
In cases where USG was inconclusive, MRI was done to visualise Mullerian structures, gonads and renal anomalies. Laparoscopy and hysteroscopy was also done for diagnosis and management as and when indicated. Cytogenetic study for karyotype detection was done in cases of primary gonadal failure and those with symptoms of androgen excess.
The causes of primary amenorrhea are classified into four compartments based on the organs:
Compartment 1: End-organ failure or out flow tract obstruction
Compartment 2: Gonadal failure
Compartment 3: Pituitary cause
Compartment 4: Hypothalamic cause
The patients were classified into 4 groups based on the aetiology of primary amenorrhea. (TABLE 1)
Table 1.Distribution of Cases based on Etiology

Results
The analysis of 15 patients with primary amenorrhea was done and the diagnosis was made on the basis of all medical records available. The etiological factor in 15 patients is given in (Table 1). The common causes of primary amenorrhea were Mullerian anomalies (9 cases, 60%), 2 cases (13.33%) of early gonadal failure, 1 case (6.66%) of pure gonadal dysgenesis, 1 case (6.66%) of Turner mosaic, 1 case (6.66%) of Androgen insensitivity syndrome (AIS, 46,XY) and 1 case (6.66%) of congenital adrenal hyperplasia.
All patients with gonadal dysgenesis and those required were subjected to cytogenetic study by karyotyping. There was 1 case of 46,XX (pure gonadal dysgenesis), 1 case was of 46,XY (androgen insensitivity syndrome) and 1 case was 45,XO/46,XX (Turner mosaic). Age at presentation for primary amenorrhea ranged from 14 to 30yrs. Maximum number of patients belonged to the in the age group of 14-20yrs as shown in (TABLE 2).
Three patients were married at the time of presentation and the rest were unmarried. Married individuals presented with complaints of infertility (20%).All the patients presenting early came with complaints of not attaining of menarche (46.66%) as shown in (TABLE 3). One patient presented with short stature, webbed neck and wide spaced nipples. On cytogenetic analysis it showed 45,XO/46,XX. Two cases presented with virilising symptoms of which one was diagnosed to have androgen insensitivity syndrome and the other as congenital adrenal hyperplasia.
A patient of Mullerian agenesis presented with pain abdomen in emergency which on USG was found to be a twisted ovary. One unmarried sexually active patient presented with vaginitis.
Table 2. Age wise Distribution of Cases
| Age group | No. of Cases(15) | Percentage |
| 14-20 | 9 | 60% |
| 21-25 | 4 | 26.67% |
| 25-30 | 2 | 13.33% |
Table 3. Symptoms At Presentation
| Symptoms | No. of Cases(15) | Percentage |
| Not attained menarche | 7 | 46.67% |
| Infertility | 3 | 20.00% |
| Virilism | 2 | 6.66% |
| Vaginitis | 1 | 6.66% |
| Pain abdimen (overian torsion ) | 1 | 6.66% |
| Short Stature | 1 | 6.66% |
Discussion
Age at menarche has been following a steady decline in the past few decades with girls attaining menarche at a mean age of 12.5yrs in India. 14 Awareness regarding the problems associated with not having attained menarche is also increasing. 15We did not see any patients in the age group 30 to 40 years because most of the inquisitive patients are diagnosed by then or have lost hopes of receiving treatment.16
We have studied all etiological aspects of primary amenorrhea in this study and determined that the most common etiological causes of primary amenorrhea are Mullerian agenesis (60%) and hypergonadotropic hypogonadism (33.33%) in this study group. Genotyping was performed in patients who got the indication, and revealed abnormalities in 2 (13.33%) cases.
Short stature was limited to the group of hypergonadotropic hypogonadism indicating hypoestrogenism. Symptoms at presentation surprisingly varied from not attaining menarche to primary infertility. According to most of the literature,
Table 4. Comparision of Our Study with other Studies:
| Etiology of Primary Amenorrhea | Present Study (2018-15 Cases ) | GS Anitha et al (2015-40 Cases) | Kumar et al (1998-48 Cases) | Pourafkari et al (2008-53 Cases) | Ratianachaiyasont M et al (1997-101 Cases) |
| Mullerian agenesis | 60.00% | 32.50% | 54.20% | 26.40% | 39.45% |
| Hydergonadotropic hypoestrogenism | 33.33% | 32.50% | 16.60% | 15.10% | 32.69% |
| Androgen insensitivity Syndrome | 6.67% | 7.50% | 0.00% | 1.90% | 3.96% |
| Others | 0.00% | 32.50% | 29.20% | 56.60% | 23.90% |
gonadal dysgenesis is the most common cause of primary amenorrhea. But, now the number of cases of MRKH is on the rise probably because more girls are ready to get themselves surgically treated and also the popularity of the surgical facilities available. Most important aspect is to do the procedure of vaginoplasty when the patient is mentally prepared and to keep the patient motivated to undergo postoperative vaginal dilatation.17 Pubertal girls should have regular follow up for individualising the management and counselling.
In cases of hypogonadotropic hypogonadism, counselling the patient regarding estrogen therapy, the risks and benefits must be explained. It is important to start estrogen therapy to bring about development of secondary sexual characteristics, prevent bone demineralisation and also to keep the uterus in a functional state for the theoretic possibility of a surrogate pregnancy with donor ovum .18 In the Table 4, we have compared our study with other studies. We have considered two Indian studies and two foreign studies. Pourafkari et al is an Iranian study of 53 cases in 2008 which highlights the use of ultrasound in the diagnosis of primary amenorrhea.15 Rattanachaiyanont et al, was a retrospective study of 101 cases done in Thailand.6
Conclusion
Primary amenorrhea work up may seem to be complex, nevertheless a well elicited history, carefully conducted physical examination followed by use of imaging modalities and bioassays for endocrine abnormalities, permitted the clinician to narrow the diagnostic possibilities andreach an accurate diagnosis quickly that helped in choosing the appropriate management option. Primary amenorrhea affects physical, mental, psychological and social life of the patient, so team approach involving gynaecologist, geneticist, psychologist and paediatrician is required.
While managing the case counselling of the patient and her near relatives is very essential for a fruitful outcome. Treatment and prognosis in terms of future fertility depends on the primary aetiology of amenorrhea. Women require long term follow up by practitioners to monitor therapies, and also to address complications.
References
- Speroff L, Marc A. Fritz. In: Clinical Gynecologic Endocrinology and Infertility. 8th ed. USA: Lippincott Williams and Wilkins; 2011. Amenorrhea; 435-493.
- Rajangam S, Nanjappa L. Cytogenetic studies in amenorrhea. Saudi Medical Journal. 2007; 28(2): 187 – 192.
- Dutta UR, Ponnala R, Pidugu VK, Dalal AB. Chromosomal abnormalities in amenorrhea: a retrospective study and review of 637 patients in south India. Arch Iran Med 2013;16(5):267-70.
- Mohajertehran F, Ghodsi K, Hafizi L, Rezaee A. Frequency and the type of chromosomal abnormalities in patients with primary amenorrhea in northeast of Iran. Iran J Basic Med Sci. 2013; 16(4): 643-7.
- Alka Kriplani a, Manu Goyal b, Garima Kachhawa a, Reeta Mahey a, Vidushi Kulshrestha a. Etiology and management of primary amenorrhoea: A study of 102 cases attertiary centre. Taiwanese Journal ofObstetrics &Gynecology 56 (2017) 761-764
- Rattanachaiyanont M, Kunathikom S, Angsuwattana S, Techatraisak K, Mekmahan O et al. Primary amenorrhoea: a retrospective study at Siriraj Hospital. J Med Assoc Thai. 1997; 80(10): 619-25.
- Jyothy A, Kumar KS, Swarna M, Raja Sekhar M, Uma Devi B, Reddy PP, et al. Cytogenetic investigations in 1843 referral cases of disordered sexual development fromAndhra Pradesh, India. Int J Hum Genet 2002;2:55-9.
- Eren E, Saglam H, Cakir ED, Tarim O. Etiological evaluation of adolescents with primary amenorrhea. Ind J Paed 2014;81:861-
- Geckinli BB, Toksoy G, Sayar C, Soylemez MA, Yesil G, Aydın H, et al. Prevalence of X- aneuploidies, X-structural abnormalities and 46,XY sex reversal in Turkish women withprimary amenorrhea or premature ovarianinsufficiency. Eur J Obstet Gynecol ReprodBiol 2014;182:211-5.
- Schorge JO, Schaffer JI, Halvorson LM, Hoffman BL, Bradshaw KD, Cunningham FG. Amenorrhea. In: Schorge JO, Schaffer JI,editors. Williams gynecology. New York, NY: McGraw Hill; 2008. p. 1112-28.
- Reindollar RH, Tho SPT, McDonough PG. Delayed puberty: an update study of 326 patients. Trans Am Gynecol Obstet Soc 1989;8:146-62.
- Reindollar RH, Byrd JR, McDonough PG. Delayed sexual development: a study of 252 patients. Am J Obstet Gynecol 1981;140:371- 80.
- Tanmahasamut P, Rattanachaiyanont M, Dangrat C, Indhavivadhana S, Angsuwattana S, Techatraisak K. Causes of primary amenorrhea:a report of 295 cases in Thailand. J Obstet Gynaecol Res 2012;38:297-301.
- GS Anitha, KK Tejeswini, Geetha Shivamurty. A Clinical Study of Primary Amenorrhea. JSAFOG 2015. 10.5005/jp- journals-10006-1348
- Pourafkari M, Ajori L, Fallahian M, Moghimi M, Azizi F. Ultrasonographic findings in a group of Iranian patients with primary amenorrhoea. Iran J Radiol 2008;5(2):97-100.
- Kumar A, Mittal S. Primary amenorrhoea (analysis of 48 cases). J Indian Med Assoc 1998 Apr;96(4):119-120.
- Vijayalakshmi J, Koshy H, et al. Cytogenetic analysis of patients with primary amenorrhoea. Int J Hum Genet 2010;10(1-3):71-76.
- Kalavathi V, Chandra N, Nambiar GR, Shanker J, Sugunashankari P, Meena J, et al.Chromosomal abnormalities in 979 cases of amenorrhea: A review. Int J Hum Genet. 2010; 10: 65 – 69.