")
Original Article
BONE MARROW STUDY IN A TERTIARY CARE HOSPITAL, ELURU- ASRAM
Lalitha S M1,Asha T2,Priyanka A A3
1Final yearPostgraduate, Department of Pathology, ASRAM Medical College 2 Professor and HOD, Department of Pathology, ASRAM Medical College 3Assistant professor, Department of Pathology, ASRAM Medical College
*Corresponding Author
Dr.ThotaAsha,Professor & HOD
ASRAM Medical College,Eluru
,West Godavari, Andhra Pradesh
Email id-thotaasha52@yahoo.com
Abstract
Introduction: Examination of bone marrow aspirate (BMA) and bone marrow biopsy (BMB) are essential for the diagnosis of bone marrow pathology. Bone marrow examination will give information about hemopoietic tissue in various conditions in addition to findings of blood sample as the bone marrow can be affected by both hematological and non-hematological disorders.
Aim and Objectives: To analyze the cause of hematological, non-hematological disorders and to interpret the bone marrow findings with various conditions.
Methods:A retrospective and prospective study of 112 patients over a period of two years (June 2015 to July 2017). Clinical details and ethical clearance from institute were obtained. Three modalities peripheral smear(PS), BMA, and BMB were used for diagnosing hematological and non-hematological disorders were included in the study.
Results: Out of 112 cases studied 68(60.7%) were male and 44(39.3%) were female with age group ranging from 3 to 82 years. In both aspiration and biopsy most common findings were Reactive marrow (25.0%), Megaloblastic anemia (20.5%) 2 (1.7%)biopsy samples were found to have Metastasis and 1 (0.8%) case was of SLE.
Conclusion: Bone marrow study is highly informative diagnostic test procedure in evaluating hematological, non-hematological disorder. The final interpretation requires the integration of PS, BMA, and trephine biopsy findings together with the results of supplementary tests such as immunophenotyping, and molecular genetic studies as appropriate, in context of clinical and diagnostic findings.
Keywords: Peripheral smear, Bone marrow aspirate, Bone marrow biopsy.
Introduction
Bone marrow examination by aspiration & biopsy is simple, cost effective, outpatient procedure & complimentary to each other. Evaluation of hematological &non- haematological disorders, even after detailed clinical history, physical examination & peripheral blood analysis the diagnosis is cryptic & crucial. This study was conducted to evaluate bone marrow samples received at a tertiary care center in our hospital over a period of two years.
Methods:
A two year (June 2015 to July 2017) retrospective and prospective study of 112 patients. Clinical details and Institutional ethical clearance obtained. As per International council for standardization in hematology guidelines, all three modalities :Peripheral smear (PS), Bone Marrow Aspiration (BMA), Bone Marrow Biopsy (BMB), performed to diagnose hematological and non haematological disorders. The bone marrow examination done under local anesthesia by the conventional technique using Jamshidi needle from the posterior superior iliac crest. BMA was done for majority of the cases. BMB was done for all cases, including the cases where aspiration failed.
Exclusion criteria:
Patients with severe thrombocytopenia or functional platelet defects, Prolonged PTINR, Severe bleeding, Children below 3years of age.
Results:
From June 2015 to May 2017, 112 patients enrolled for the study.
Table.1 Age distribution
| Age distribution | N(112) | % |
| <15 years | 12 | 10.7 |
| 15-30 years | 23 | 20.5 |
| 31-45 years | 26 | 23.2 |
| 46-60 years | 37 | 33.0 |
| 61& above | 14 | 12.5 |
| 112 | 100% |
Table 2. Presenting complaints
| Presenting complaints | N(112) | % |
| Fever of unknown origin | 32 | 28.5 |
| Generalised weakness | 24 | 21.4 |
| Weight loss | 19 | 17.0 |
| Organomegaly | 19 | 17.0 |
| Others | 18 | 16.0 |
Table3. Peripheral smears
| PERIPHERAL SMEAR | N(112) | % |
| Pancytopenia | 52 | 46.4 |
| Anemia | 31 | 27.7 |
| Leukemia | 16 | 14.2 |
| Bicytopenia | 7 | 6.2 |
| Sub leukemic leukemia | 6 | 5.3 |
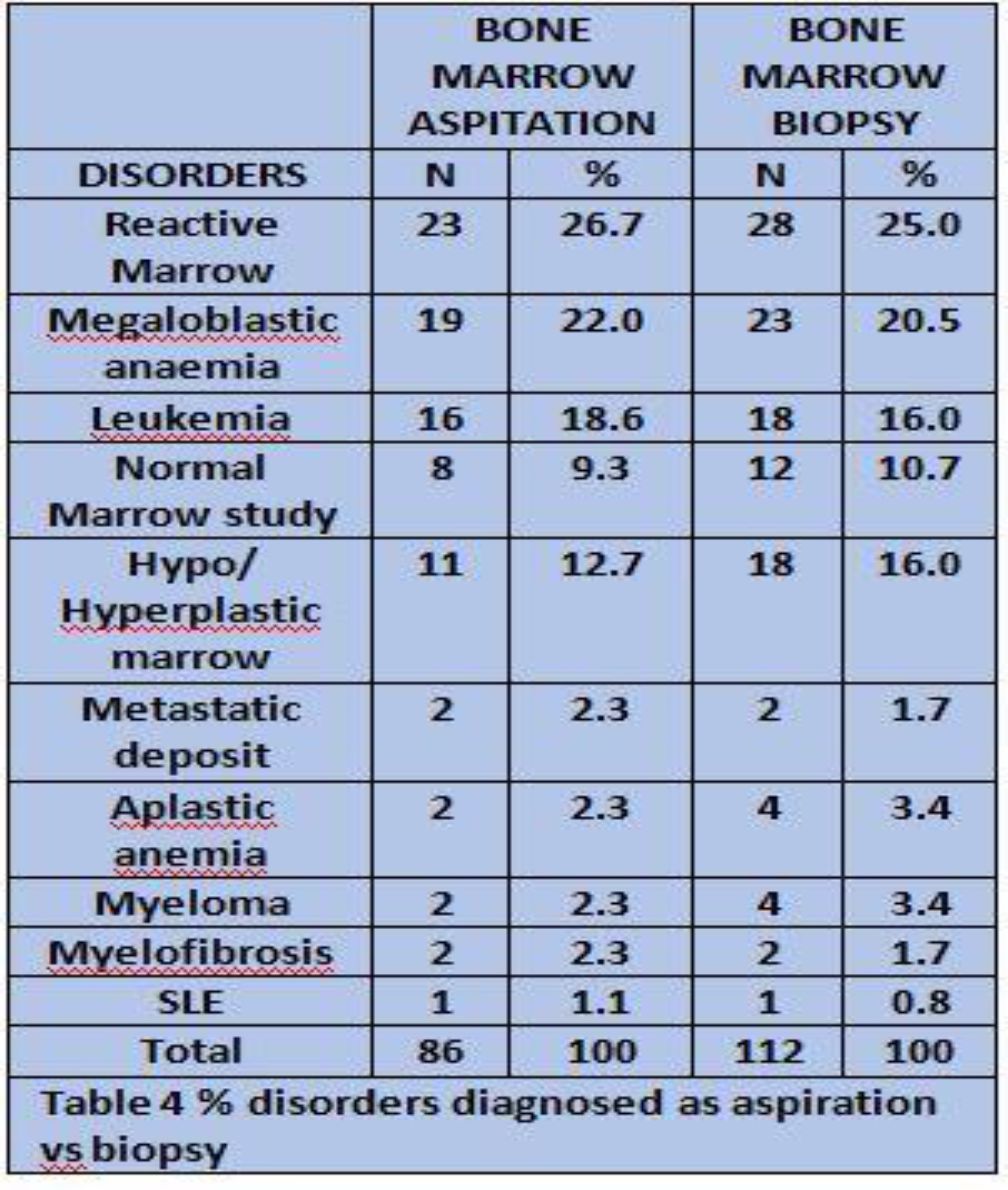
| BMA & BMB | N(112) | % |
| REACTIVE MARROW | 29 | 27.1 |
| MEGALOBLASTIC ANEMIA | 23 | 20.5 |
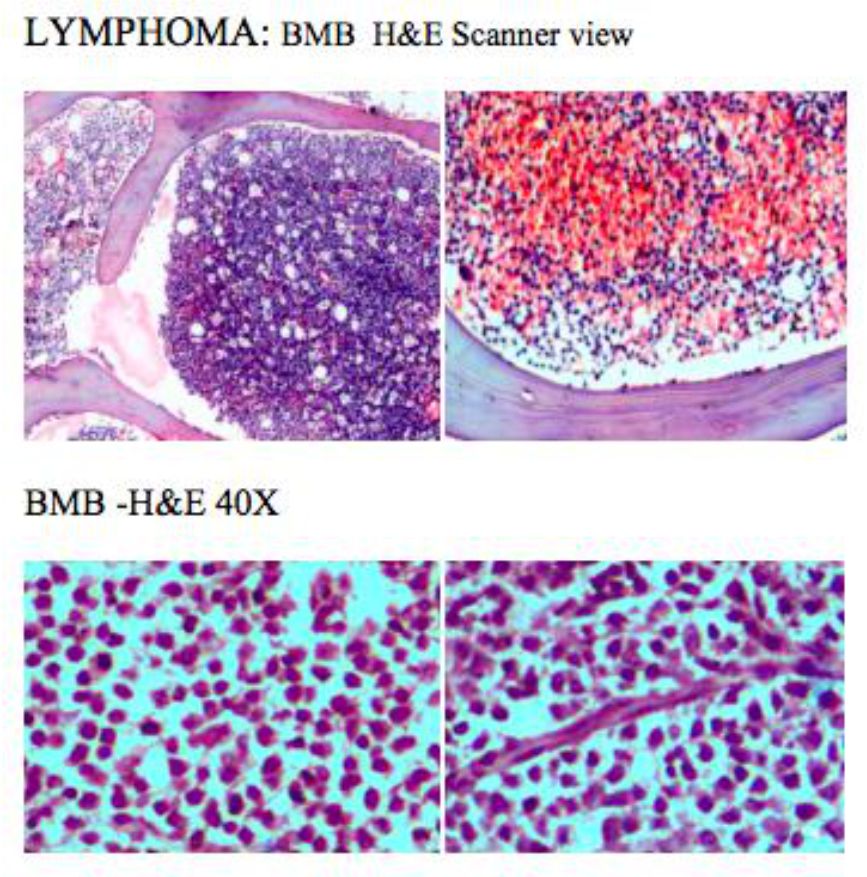
| LEUKEMIA/ Lymphoma | 18 | 16.8 |
| NORMAL MARROW STUDY | 18 | 16.8 |
| OTHERS | 11 | 10.2 |
| APLASTIC ANEMIA | 4 | 3.7 |
| MYELOMA | 4 | 3.7 |
| TOTAL | 107 | 100% |

Discussion:
| No | Study | Year | No of Cases | Percentage |
| 1 | Tilak Et Al | 1999 | 77 | Megaloblastic Anaemia (68%) |
| 2 | Khodke Et Al | 2001 | 50 | Megaloblastic Anaemia (44%) |
| 3 | Shilpa Patel Et Al | 2014 | 34 | Megaloblastic Anaemia (28%) |
| 4 | Present Study | 2017 | 112 | Megaloblastic Anaemia (20.5%) |
Table 6 showing the previous studies.
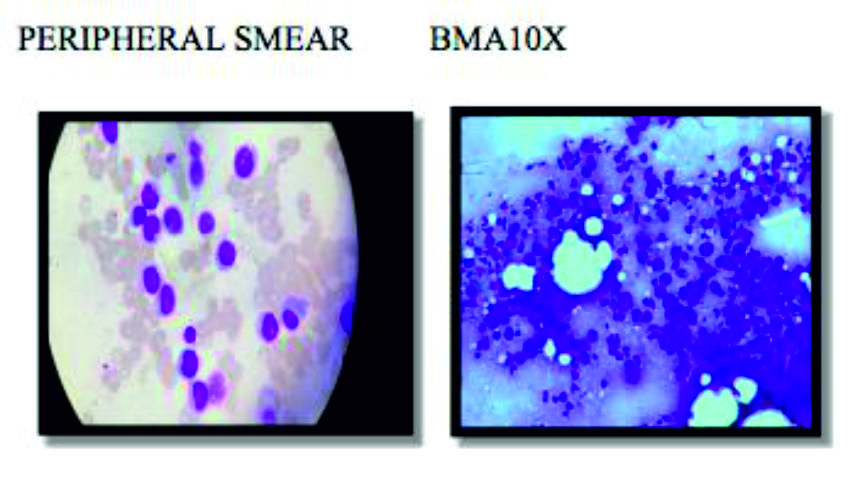
MEGALOBLASTIC ANEMIA:
Megaloblastic anemia is 20.5 % in our study and these results are in comparison to the study by shilpa et al. However, the other studies such as Tilak et al and Khodke et al reported 68% and 44% of megaloblastic picture.
LUEKEMIAS:
As per Islam A and Frisch B et al: Bone marrow histology is often supplementary investigation in acute myeloid leukemia. However, when peripheral blood features are not diagnostic, and bone marrow aspiration is unsuccessful BMB is needed. Our study has similar outcome.

MYELOMA:
Bone marrow biopsy is recommended in multiple myeloma even if an adequate aspirate as a baseline to assess a post treatment response as per Smith Et AL. There were 4 cases (3.7%) of myelomas in our study two of them were diagnosed on biopsy where aspiration yielded a dry tap. Bone marrow biopsy was done in all four cases.

METASTASIS:
In 2 known cases of multiple metastasis marrow examination was advised to evaluate refractory anemia, marrow biopsy revealed deposits. In our study out of 1.7 % cases of metastatic tumors, One case was SCC, another case was diagnosed to be Adenocarcinoma on biopsy. When compared with Nandu et al 2.8% and Toi et al 2.6% metastatic deposits respectively.


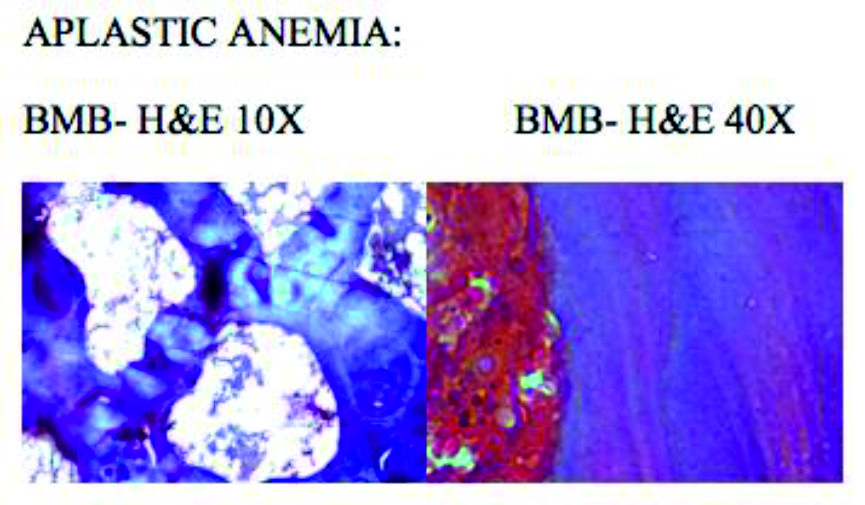
APLASTIC ANAEMIA:
| Sr No | STUDY | % | BMA/BMB |
| 1 | International Agranulocytosis and Aplastic Anaemia Study7 | 52.7 | Aplastic Anaemia |
| 2 | Verma Et Al | 40.0 | Aplastic Anaemia |
| 3 | Present study | 3.5 | Aplastic Anaemia |
APLASTIC ANEMIA:
Our study reported only 3.5% of aplastic anemia picture, whereas the other studies have reported more than 40% as shown in above table.
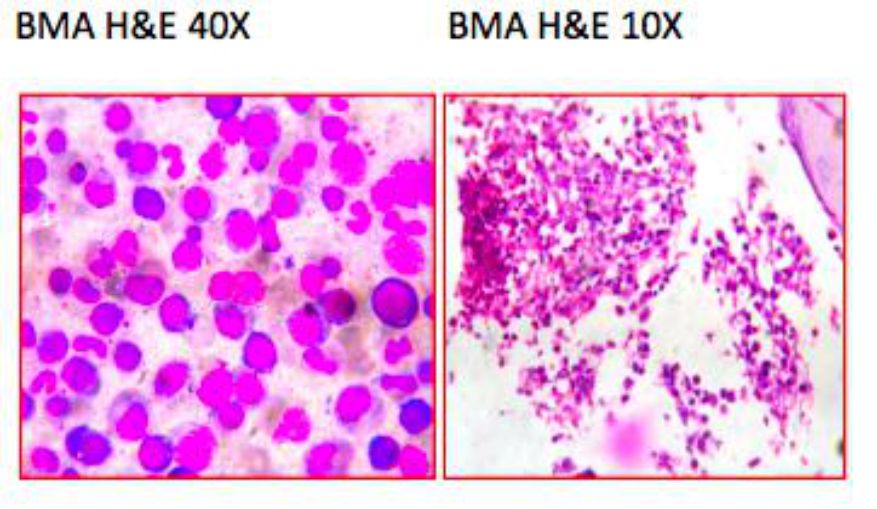
PERIPHERAL SMEAR BMA10X
Conclusion:
Peripheral Smear findings provide valuable information in planning for further investigations. BMA & BMB are valuable and usually complement each other. BMA smears are ideal for cytomorphology of hematopoietic cells. Nutritional anemias and hematological malignancies are readily diagnosed by BMA. BMB helpful to assess cell type, cellularity, extent and pattern of tumor infiltration. BMB can diagnose SLE, hypoplastic or aplastic anemias, myelofibrosis, lymphomatous infiltrations, myeloma and metastatic deposits.
References
- ICSH guidelines for the standardization of bone marrow specimens and reportsS.-H. LEE*, W. N. ERBER†, A. PORWIT‡, M. TOMONAGA§, L. C. PETERSON– FOR THE INTERNATIONAL COUNCILFOR STANDARDIZATION IN HEMATOLOGY
- Pudasaini S, Prasad KBR, Rauniyar SK, Shrestha R, Gautam K, et al Inter pretation of bone marrow aspiration in hematologicaldisorder
- Dr. Shilpa Patel, Dr. PoojaNathani, Dr.Nailesh Shah,Dr.C.K.Shah. Diagnostic Role of Bone Marrow Aspiration and Trephine Biopsy in hematologicalpractice.
- Tilak N, Jain R. (1999). Pancytopenia – a clinicalhaematological analysis of 77 cases. Indian journal ofPathology and Microbiology; 42: 4: p 399 – 404.
- Khodke K, Marwah S, Buxi S et al. (2001). Bone marrowexamination in cases of pancytopenia. Indian Academy ofClinical Medicine journal; 2: p 55 – 59.
- Hossain MA, Akond AK, Chowdhary MK etal. (1992).Pancytopenia – a study of 50 cases. Bangladesh Journal ofPathology; 1:p9–12.
- Verma N Dash S. (1992). Reappraisal of underlyingpathology in adult patients presenting with pancytopenia.Trop Georg Med; 44: p 322 – 327.
- Nanda A,BasuS,MarwahaN.Bone marrow trephine biopsy as an adjunct to bonemarrowaspiration.JAPI 2002;50:893- 5
- ToiPC,Varghese RB, RaiR.Comparative evaluation of simultaneous bone marrow aspiration and bonemarrowbiopsy.An institutional experience. Indian J Hematol blood transfusion 2010;26:41-4.
- Keisu M, Ost A. (1990). Diagnosis in patients with severepancytopeniasuspected of havingaplastic anaemia. EurJHaematol: 45: p 11– 14.
- International agranulocytosis and aplastic anaemiastudy.Incidence of Aplasticanaemia, the relevance of diagnosticcriteria. Blood (1987); 70: p 1718 – 1721.
- Journal of Pathology of Nepal (2012) Vol. 2, 309 -3124. B J Bain. Bone marrow aspiration.JClin. Pathol 2001;54:657-663
- Islam A, Frisch B and Henderson ES (1989) Plastic embedded core biopsy : a complementary approach to bonemarrow aspiration for diagnosing Acute myeloid leukemia.Jclinpathol 42,300-306
- Islam A, catvosky D, Goldman JM and GaltoDAG(1985),Bonemarrow biopsy changes in acute leukemia.I :observations before chemotherapy.Histopathology.9,939-957.